
Original article
The Sinus Approach by A Taper Osseoü]tome & Spreading Method with WIDE BASEüiHAü]surface) Implant VS Standard Implant.
May2002 - April2005 Clinical Research.
New York University college of Dentistry
Continuing Dental Education Programs
MAY 2005
Continuing Dental Education Programs
MAY 2005
Key Words: Non Drill, Layer graft, WIDE tapered, HA coat, Compression Osteo-tome.
SUMMARY
We still have many problems in placing implants on maxilla molar area. In this study New 5.5mm platform tapered HA coated implants were used with crestle sinus lift osteotome technique to compared by standard (3.7-4.2mm) Implants for control.These new Implants (n=113) were high success rate (99.1%) in short-term (7month~3years).
In particular, we have found that was achieved for short heights of original bone in maxilla molar areas (Average 4.0mm for tapered vs. average 6.9mm for control).However there is no measurement on how much to lift the membrane between both implants (Average 6.6mm for tapered vs. average 6.3mm for control).
In addition, previous methods of the layering technique on HA coated implant surface with Autogenous bone graft or synthetic graft material were found to be a safe && secure method histologically and clinically in order to prevent Schneiderian membrane perforation and to promote early osseintegration.
Notes
Except figure 42, 43. Data, Chart , Drawing , Case photography, Staining section photography.ü@All figures were made by EIJI KATO D.D.S ( ITDNü]Tokyo) .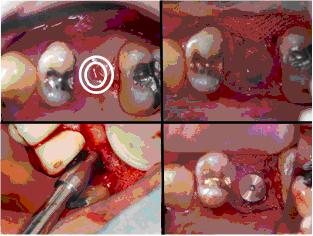
- Fig1ü]2
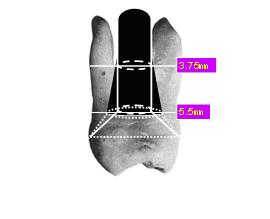
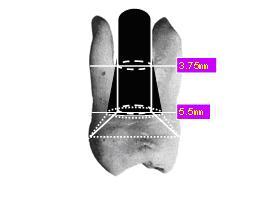
- It is difficult to have a proper emergence profile for molars with a standard (3~4mm) platform implant. A bigger inter proximal space, had that allows food impaction is usual. Also, if the patient has a wide smile, or if a patient has had premolars extracted, due to orthodontics, their black triangle causes esthetic problem.
To fill this space prosthetically, it might cause biological width invasion or an unhygienic crown. According to KAMIJO, the average distance of 1st molas teeth of Japanese mesio-distally is 10.6 mm and bucco-lingually 11.3 mm.
If the 3.75mm platform is at crestal level, it needs the angle of 42ü]48üŗto achieve proper anatomy at the occlusal plan level. However, if a 5.5mm platform is used, the angle can be 50ü]56üŗto achieve a natural tooth emergence profile .
I. Purpose
Clinically, a safe and simple method of bone regeneration is needed. Also, we need a biological, functional biomaterial with better configuration.However, many problems yet exist in placing implants on the maxilla molar area.
Sinus elevation, by using lateral window technique with autogenous graft, allograft, xenograft or synthetic bone, has been successfulüDHowever it has not become a standard, because perforation of sinus membrane is a risk and the operation is complicated.
On the other hand, the Osteotome technique has its problems, such as perforation of the sinus membrane with extensive tapping or poor primary stability.
Therefore, we have modified the implant placement procedure, fixture surface texture, and graft configuration.
In this study, we have investigated the possibility of these techniques by comparing Osteotome techniques by evaluating the bone height and collecting Pre & Post operative data.

II. Material and Methods
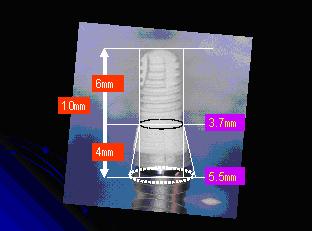
Since May 2002 to Sep 2004, 113 NEW TYPE WIDE IMPLANT( Kyocera ,JMM) 5.5mm (platform)diameter tapered implantü@have been placed.This Implant has a 20ā╩thickness HA layer which is sprayed at 2000 degree Celsius. In cases with poor quality or quantity of bone, CT scans were a taken and were analyzed with SIMPLANT software (Materialize). Two techniques were used to place implants in this study using. Tactile sense; 1) Drilling technique or 2) Spreading technique. The drilling technique was used in bone type II or III(Lekholm & Zarb), whereas the Spreading technique was used in bony type III or IV.
Drilling was performed 2mm below sinus cavity and an osteotome was used to widen the hole up to 3.4mm diameter using either manual pressure or a mullet technique. The sinus floor was then elevated and with a 2mm of bone plug and spread with newly designed instrument (PRE WIDE FORMER).
HA (OsseogratSD Kyocera ,JMM) particle were first grafted into the cavity. Then a trial guide pin was inserted, and x-ray was taken to confirm that the floor was raised without perforation.
Then a second grafting layer of ā└-TCP(Osfarion OLYMPUS) particles were inserted into the cavity.
Finally, autogenous bone graft (maxillofacial) was inserted to the cavity for direct contact with the fixture.
The fixture was then stabilized in a self-tapping fashion.
Wide Implants with HA coated surface were mostly used in the maxilla molar area.ü@In the mandible molar area, a standard type of implant was mostly used because of the bucco-lingual width after bone loss. In cases with poor bone quality, primary stability was not easily achieved with a standard drill technique.
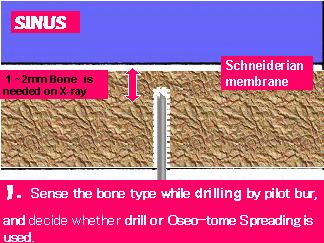
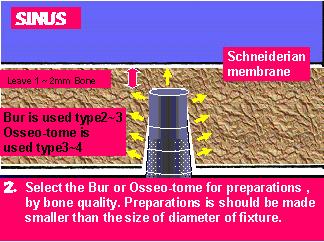
- Fig6ü]7
- In this case with type III or IV bone, bone spreading was performed up to 3.4mm using osteotome illustrated in Fig 8, after a pilot drill was used to widen up to 1.6mm.

- Fig 8
- BOSTOME II)
Diameter 1.6mm -> 2.3mm
Diameter 2.2mm -> 2.9mm => 3.2mm Fixture
Diameter 2.8mm -> 3.4mm => 3.7mm Fixture
Diameter 3.3mm
Statistics:
Panoramic x-rays ( PANORA YOSHIDA)of 1.2x magnification were used to measure both the preoperative bony height and postoperative bony height.ü@If there was 4-10mm of original bony height, one stage surgery was possible when wide implant and osteotome technique were used. When more bony height was needed, a one stage lateral approach or multiple osteotome techniques were used. In cases with 1-3mm of original bony height, 1 mm of bone loss could be expected and a one stage surgery was not possible.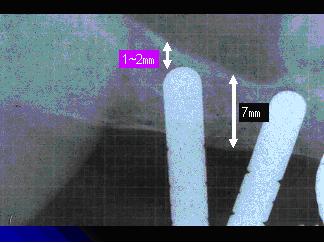
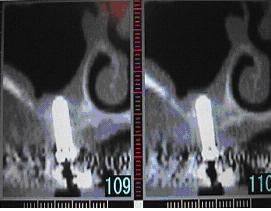
- Fig 9
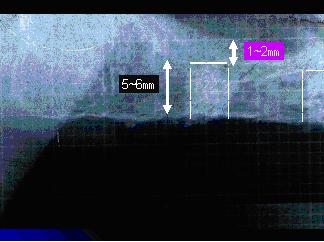
- While between operative, P-A X-rays was used confirm of remain bone within trial guide.
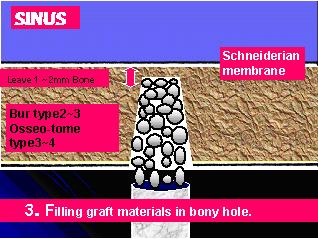
- Fig10ü]11
- At first, bone graft material with high density is filled flash with osteotomy.
Operation concerns:
- A tip of an instrument such as a drilling bur or osteotome should not enter the sinus cavity.
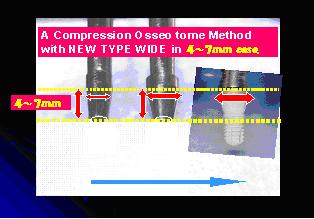
- Minimum of 4 mm of original bone height is needed. Sinus floor can be raised by 6-7mm maximum. for one stage surgery.
- In cases with 1-3mm of original bone height, one stage surgery was not possible because 1mm of bone loss of the anticipated (w/o implant placement)
- In cases with less than 3-4mm of original bone height, a double osteotome technique is used for future implant site development. In this technique, drilling with a 5mm diameter trephine bur at 2mm depth is done followed by raising the sinus floor. An implant is placed after 6 months.
- X-ray are taken three times;ü@In the 1st Osteotomy with a trial pin; When the graft material is placed; After placing an implant.
- In case with discrepancy of height at sinus floor mesio-distally, the narrowest osteotome is used to raise the floor.
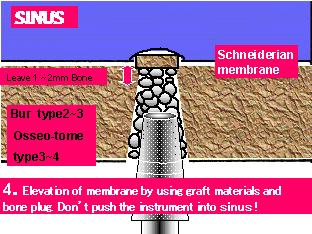
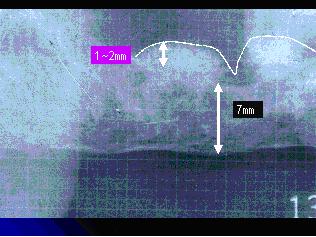
- Fig12ü]13
- Oseotome with measurement scale, the scale is used to lift the material up to the height of original bone with bone plug. 1mm of lift is possible with one operation.
Several operation are repeated. Then, check if there is perforation of membrane with X-ray.
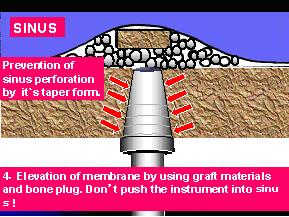
- Fig14-15
- After lifting Schneider membrane, tapered osteotome is used to modify the cylindrical osteotomy which was already made. Finally, tapered implant is self tapped
- Fig16
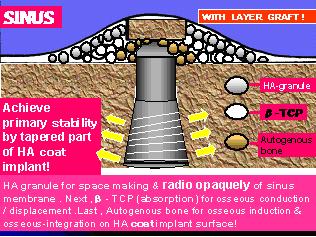
- Primary stability is achievedü@with the tapered position of implant.

- Fig17-19
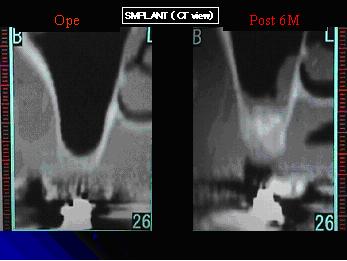
- If there is no perforation, dome-shaped elevation can be confirmed when a HA granule is placed right under Schneiderian membrane.
Autogenous bone graft around a fixture is remodeled so that it becomes rodiooparue low radiolucent tissue after 6month of process .

- Fig20
- In precedence clinic before marketing 02' April to 04 'Sep for 28month, we have placed mostly 10mm length, Tapered 5.5mm diameter HA prototype Implant.
Total placement including standard type implant were placed mostly at mandible molar area .
On the other hand, there was much wide implant in maxilla molar part. Because bucco-lingual width at mandible molar area is narrow.
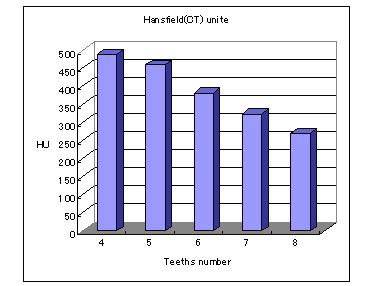
- Fig21
- Hansfield units value lowered down gradually on the distal side of maxilla molar area.
It indicates that the bone density is low and bone is soft.
III. Results
As a control, the drill technique in the lower molar area, ( bone type II or III) was selected. In maxilla molar area with bone type III or IV, the Spreading technique was used.In post-operatively, X-rays were taken for the check. A Perio Test (SEMENS) was used to evaluate mobility. No more than 2mm of bone loss was noted from 5 to 36months post-operatively. One case exhibited bleeding and mobility of the implant due to malocclusion seen at the time of stage II, but the final restoration was placed after 6 months. One fixture that was removed due to mobility 5 months after the final restoration.
Both implant types showed an average gain of about 6mm of bony height. No significance was noted compared to standard implants where the original bony height was 6.9mm. On the other hand the 4.0mm WIDE implants showed significance in bony heights.
The Wide implants were more successful in comparison with the standard implants even in cases with thinner original bone height.
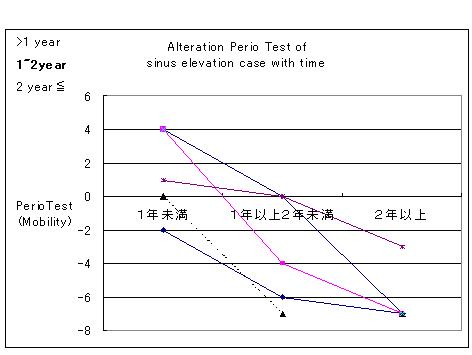
- Fig22
- A mobility ofü@using Perio Test (SEMENS) is stable with time.
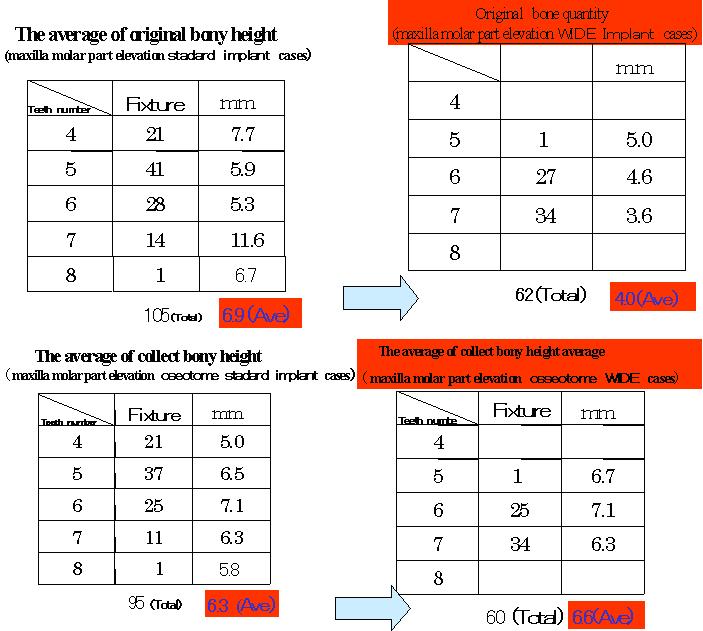
Notes : Fig of collect height
10 standard implants and 2 wide implants were excluded, because did a lateral window technique.
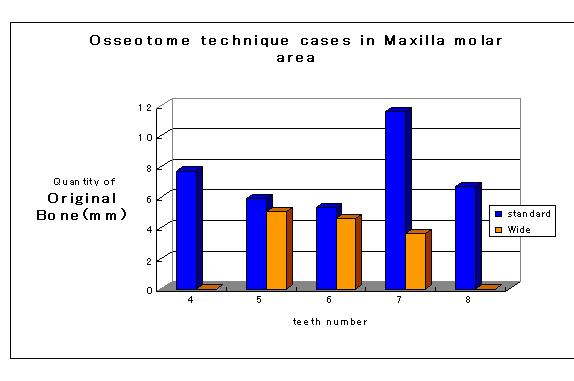
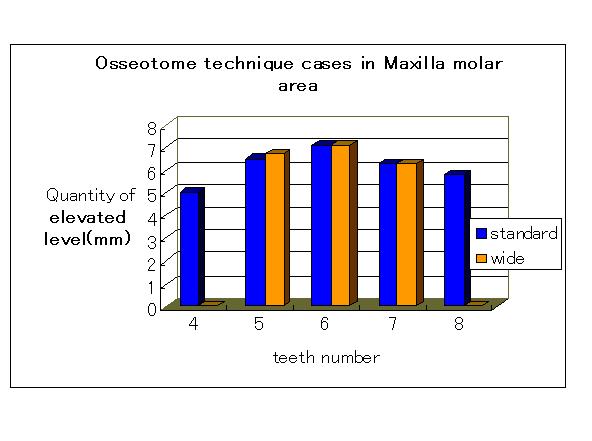
- Fig25-26
- A comparison of original bone height in this study, between standard 3.7-4.2mm and wide tapered Implant 5.5mm.ü@Wide implants were used often at shot bony height. However, the amount of elevation did not make a difference.
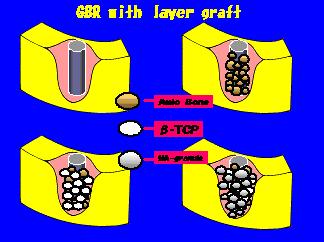
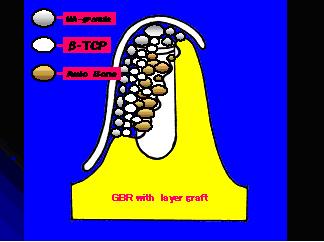
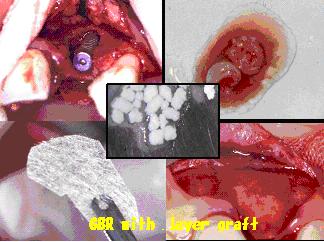
- Fig27-29
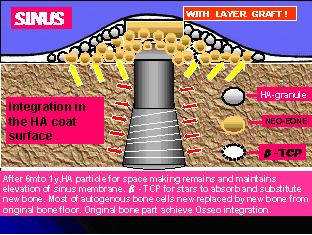
- GBR technique with Sinus elevation technique. An autogeneus graft is used around implant distant from pristine bone for osseoinduction and osseointegration.
Resorbable bone graft is then filled around the autogeneous graft. Non-resorbable graft material is also used to maintain the membrane for space maintaining.
Also Non-resorbable Material is used to maintain the membrane for creating space.
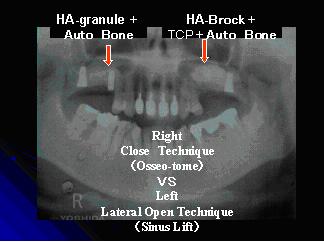
- Fig30
- Right side:
Osteotome lift ;HA particle graft was placed first, then autogenous bone graft particle was placed. Finally, fixture was inserted.
Left side:
Lateral window Sinus lift : HA particle graft and tent pourer of HA block as a tent pole was placed first, then combination ā└- TCP and autogenous bone graft particle was placed circumferencially.
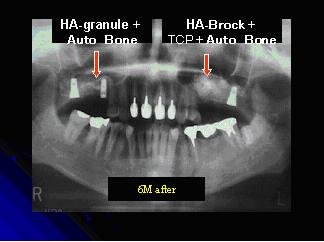
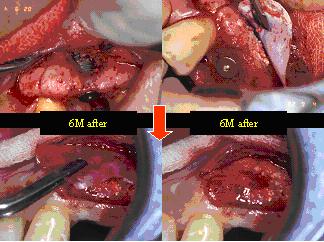
- Fig31
- 6month after;
Right side:
Level of lifted membrane has been maintained, radiolucecy is found on the area of autogenus bone graft by remodeling process.
Left side:
Level of lifted membrane has been maintained by HA block.
ā└ü]TCP & Autognus bone particle has gained more radiolucency.
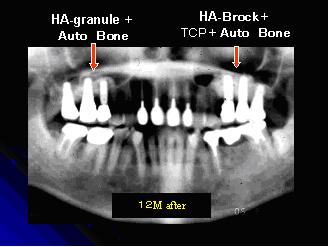
- Fig32
- 12month after;
Right side:
Level of lifted membrane has been maintained, radiolucecy is found on the area of autogenus bone graft by mature stage.
Left side:
Level of lifted membrane has been maintained by HA block.
ā└ü]TCP & Autognus bone particle has gained more radiolucency.
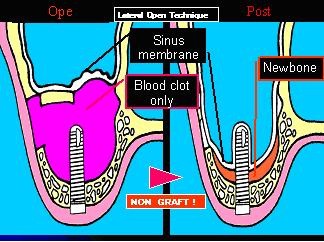
- Fig33
- Lateral approach of sinus lift:
If no graft is placed after the membrane lift, level of membrane lift is not maintained. It seems that blood clot it self healing, the regeneration of new bone is limited in 6months.
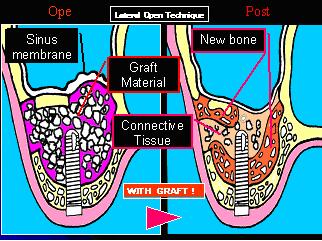
- Fig34
- Bone graft is used for space making.
However, the area which is away from cell source can not expect osseointegration .
because connective tissue surrounds graft remnants with little new bone
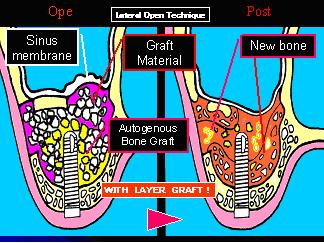
- Fig35
- Autograft is placed around implant and in the area distant from native bone to promote ostesgenesis and osseointegretion .
And resolvable graft is used for regeneration or space making.
Also non-resorbable graft is use for sinus membrane support.
- Fig36
- Autograft is placed around fixture , e-PTFE membrane is used on lateral window for barrier ā└-TCP particle .
In 6 mounths, ā└-TCP particle is still remained and replaced resolved .
- Fig37
- Staged sinus lift technique.
In 6 months, sinus membrane lift is maintained in CT scan image .
- Fig38
- Where is bone cell coming from on sinus lift surgery ? => In maxillary bone wall from native bone.In 6 months new bone is found on alveolar side, but not at the lifted membrane side.
- Fig39
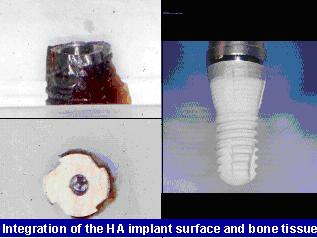
- The rough surface used was previously believed to cause peri-implantitis .
However, due to surface texture innovation, stronger osseointegration is achieved with rough surface implants than Ti-polished surface. This indicates HA as "bio-material" potency.
- Fig40
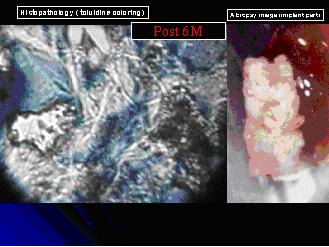
- In Toluidine blue staining, there is close contact between Ti-surface and HA coated surface.
Bone penetrations is into the inditation on HA & bone are consideration to be right contact in tight.
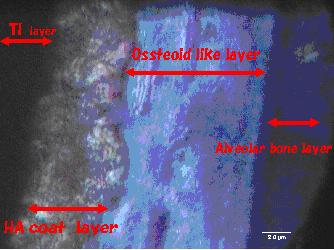
- Fig41
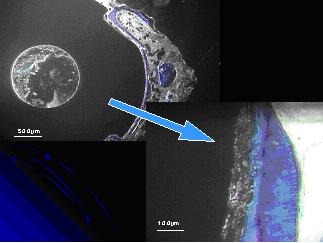
- There is 100ā╩m thickness of osteoid layer around HA coated surface. It indicates the closeü@integration of HA & Bone.
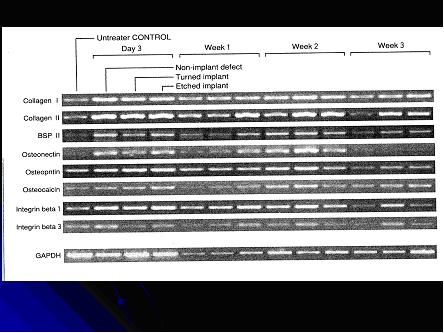
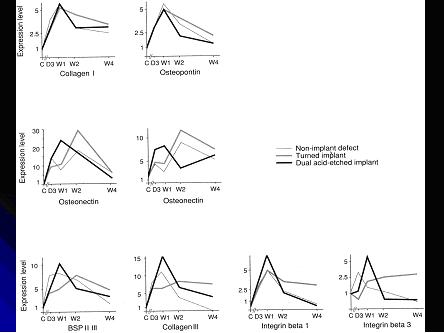
- Fig42-43
- Animal study on the healing process of drilled osteotomies using genetic analyzing.
The healing process was compared, between osteotomies with implant placed and osteotomies without implant placed . Ti-polished implants were found to have bone at an early stage of healing . In Dual acid-etched Implant placement, cytokine & intagrin, collagen , etc were found at an early stage of bone healing too.ü@ This study indicates that rough surface implant promotes bone healing.
IV. Consideration
Three things were considered to achieve successful implant osseo- integretion :(1) Primary stability was achieved by selecting the method of bony preparation depending on the bony type. It seems that wide tapered implants could gain primary stability with less bony height.
(2) Direct contact of the HA surface with autogenous graft increased osseointegration.
(3) Technique and instruments should be used to prevent perforation of the sinus membrane and the used for excessive drilling.
These considerations indicate a wider range of use of implants in the maxillary molar area even in cases makes being less bone height.
V. Conclusion
The guidelines have been expanded for cases with poor maxillaly posterior bone.In this study 99.1 % of the cases in maxillary molar implant were successfully integrated in the proper technique selection depending on original bone height.
In particular this Wide tapered HA coated implant and these utilizing new guidelines will benefit posterior maxilla of poor bone quality and quantity.
ćYüDAcknowledgement
Iü@appreciate that Assistatant Dean for C.D.E. H. Kendall Beacham and Program Director for C.D.E. Kate E. Matumoto gave me an opportunity of such a thesis presentation. And I give thanks to Dr. Dennis P. Tarnow and Dr. Stephen Wallace,they had a lot of precious lectures about a sinus operation.At last, I thank very much Dr.Takuya Kansaku and Dr.Todd Yamada for thesis fabrication and correction.
References
1) Eiji Kato et al. :The possibility of clinical use of frozen PRP, atelo-collagen, HA and cultured autogenic bone graft materials. Journal of Oral Tissue Engineering 2(1):40-60, 20042)Masahiko Kamijo:Anatomy of Japanese dentes permanents. Anatomu publishing Company,1962
3) Bony P.J.,James,R.:Grafting of the maxillary floor with autogenous marrow and bone. J Oral Surg.38:613-616, 1980.
4)Tatum H,Jr.:Maxillary and Sinus Implant Reconstruction. Dent Clin North Am.30:207-229,1986.
5)Summers,R.B.:A new concept in maxillary implant surgery:The osteotome technique,Part1-3.CompendiuContEducDent.15:152-156,422-426,698-704,1994.
6)Palti A. and Steigmann M.:Long-Term Success with Sinus Elvation-Criteria and Parameters,Int Magazine Oral Implantology 4:20-24,2003.
7)Kasabah S, Krug J, Simunek A, Lecaro MC.:Can we predict maxillary sinus mucosa perforation? Acta Medica.46(1):19-23.2003.
8)Cosci F.,Luccioli M.:A new sinus lift in conjunction with placement of 265 implants: A 6year retrospective study. Implant Dentistry.9:363-368,2000
9üjOgawa T, Ozaw S,Shih J-H, Rtu K.H, Sukotjo C, Yong J=M, Nishmura I, Biomechanical Evaluation of osseous implants having different surface topographies in rat. J Dent Res.2000; 79(11):1857-1863
10üjOgawa T, Nishmura I. Different bone integration profiles of turned and acid-etched implants associated with modulated expression of extracellular matrix genes.
11) Ogawa T, Sukotjo C, Nishmura I.Modulated bone matrix-related gene expression is associated with differences in interfacial strength of different implant surface roughness.J Prosthodont.2002;11(4):241-247
12) Eiji Kato: The new century prospects of esthetic zone reproduction From micro-instrument application to self cell culture, The Dental magazine Clinical report No108 2003
13) Eiji Kato: New concept -PRP of a reproduction treatment. Fundamental and clinical of PRP and Collagen medicine-,The Dental magazine Clinical report No102, 2002
14) Eiji Kato: For the optimal implant system. The Japan dental review No679/93-100 1999-5